Diabetic eye screening: cohort management
Updated 30 March 2026
Applies to England

© Crown copyright 2026
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: psi@nationalarchives.gov.uk.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at /government/publications/diabetic-eye-screening-cohort-management-overview/diabetic-eye-screening-cohort-management
1. Introduction
The NHS Diabetic Eye Screening Programme aims to reduce the risk of sight loss by the early detection and treatment, if needed, of diabetic retinopathy and maculopathy. Diabetic retinopathy and maculopathy are complications of diabetes, which are caused by high blood glucose levels damaging the back of the eye (retina) and can cause blindness if left undiagnosed and untreated. All people with diabetes aged 12 and over should receive regular eye screening as one of their essential free NHS checks and services.
This guidance explains how to effectively manage the groups of people eligible (cohort) for diabetic eye screening (DES) within local services, focusing on the use of electronic patient data from NHS GP practices to accurately identify and maintain these groups.
It defines the eligible population and provides clear criteria for inclusion, exclusion, and suspension from screening, while ensuring alignment with national pathway standards. The guidance also outlines protocols for managing consent and individual choice, as well as procedures for addressing specific clinical scenarios, including rare forms of diabetes, to support equitable and comprehensive screening delivery.
2. Identification of the cohort
Each local DES service is responsible for maintaining a register of individuals with diabetes who are eligible for screening, referred to as the single collated list (SCL).The population covered by this guidance includes all eligible individuals with diabetes registered with NHS General Practices, Defence Medical Service (DMS) practices, secure and detained settings, including prisons, immigration removal centres, children and young people’s secure settings and those in any other institutions. If an individual is not registered with one of these organisations it may be more difficult for them to attend screening. Local DES services should have policies in place which enables those not registered with one of the above organisations to attend to ensure equity of access to screening for underserved and vulnerable groups.
A nationally commissioned General Practice 2 Diabetic Retinopathy Screening (GP2DRS) system is used to automate the electronic extraction and secure sharing of information about people with diabetes between General Practices and local diabetic eye screening services.
This system is overseen and commissioned by NHS England. All local DES services in England are required to use GP2DRS (or any future replacement) as their primary data source for their screening cohort list. Data extracts from this system must be considered as part of any service mobilisation activity, including re-procurement or service reconfiguration.
People with diabetes must be correctly coded on their GP practice IT system with a SNOMED code to be included in future GP2DRS extracts, and for future demographic changes (e.g. address change) to be received by the service.
National Institute for Health and Care Excellence (NICE) guidance recommends all referrals for diabetic eye screening should be made immediately on diagnosis of diabetes to ensure the person has eye screening within 3 months from the service being informed of an individual’s diagnosis. GP2DRS facilitates this process. However, to ensure timely eye screening, the appropriate diabetes SNOMED codes must be applied immediately to an individual’s primary care record by their GP practice following diagnosis of diabetes.
Individuals with diabetes may also be manually referred to the local DES service where this is agreed by the local DES service. Additional information can be included on a manual referral; however, newly diagnosed service users must still receive their first screening within 3 months of the DES service being informed of their status.
3. Reconciling the single collated list/cohort
GP2DRS data is extracted each month and shared with DES services.
Services are required to promptly upload the extract to their respective screening software. A local protocol must be in place to ensure accurate and complete upload of the data has taken place in line with information governance and data protection standards. This is particularly important if the member of staff involved with the upload can access and upload more than one screening service’s cohort.
It is mandatory that local DES services perform reconciliations against their existing SCL every month.
This process must include a systematic review of all relevant GP2DRS reports and files, as outlined in the GP2DRS Support Pack guidance, and the use of embedded reconciliation tools within the screening software if available. Services are responsible for initiating the investigation of any discrepancies between the SCL and the GP2DRS extract, acknowledging differences that result from routine changes such as new registrations, deceased notifications, or demographic updates.
Where a number of individuals in the GP2DRS extract are still not recognised within the local SCL, this should be investigated further and may be treated as a potential screening safety incident and escalated in accordance with local governance procedures.
3.1 Individuals missing from GP2DRS
Individuals with diabetes who are registered within a local DES service’s SCL but do not appear within the GP2DRS extract are considered ‘missing’.
Individuals may be missing due to changes in diabetes status (i.e. the GP practice has removed a diabetes code entered in error), relocation (e.g. moved out of area), or death.
Services must conduct checks for missing individuals directly with the GP practice and determine the accuracy of their absence from the GP2DRS extract.
The DES service must review an individual’s eligibility for ongoing screening when their diabetes status changes, and diabetic retinopathy was previously detected. If the review concludes the individual should be removed from the SCL, the service must communicate this decision to both the individual and their GP. Comprehensive documentation must also be recorded in the individual’s file within the SCL prior to their deactivation from further screening.
3.2 Untraceable individuals with diabetes
Untraceable individuals are those who are no longer registered with a GP in England. Please note, individuals who are registered with a GP in England but living elsewhere for an extended period are not considered untraceable and services should continue to invite these people for screening. GP practices will provide current addresses for these people if they are notified.
If an individual is untraceable, the service must attempt to locate them by:
- contacting the last registered GP
- checking the NHS Spine and local registration systems
- check with any HES or diabetes department where the individual has had regular appointments
All actions must be recorded in the individual’s electronic record. Individuals remain eligible for screening for 12 months from the date the investigations started.
If there is no further information from the GP after 12 months and the NHS Spine does not show the individual has registered with another GP practice in England, their status should be changed to ‘off register’ due to ‘moved out of area’ with a note in the electronic record showing them as untraceable, along with details of investigations made to trace them. The service should write to their last known GP to notify them of this action. Until the individual is marked as ‘off register’ in the local services DES system, they will continue to be flagged in the ‘missing patient’ report after each monthly GP2DRS import.
4. Individual Choice for Diabetic Eye Screening (DES) location
People in England can choose their GP practice and, similarly, may opt for a different DES service than the one linked to their GP. The process that DES services must follow is detailed in the current individual choice for diabetic eye screening guidance. This guidance is under review and should be followed until it is updated.
5. Cohort descriptions
The diagram below describes the separate groups of individuals in the DES programme cohort and shows how local DES services should manage and maintain their local SCL. This diagram also supports the DES software providers to develop appropriate reports and facilitates the failsafe of people within the screening programme.
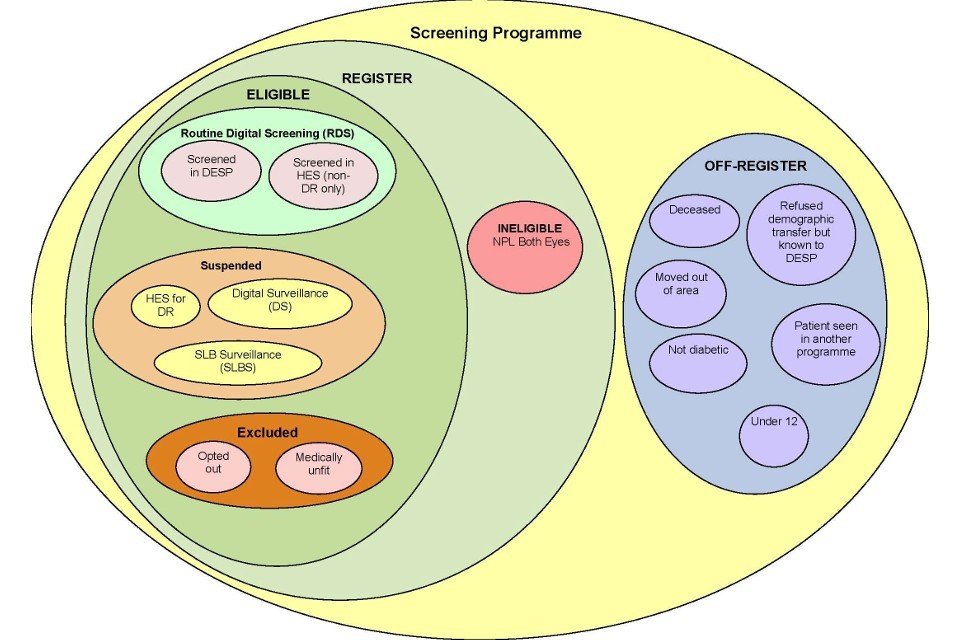
Diagram representing the cohort for the diabetic eye screening programme.
6. On register
This includes those individuals who are on the screening programme register and can be classed as eligible or ineligible for screening.
6.1 Eligible for screening
Individuals with the following classifications are eligible for screening and will appear as active individuals within the programme reports:
- routine digital screening
- screened in DES programme
- screened in HES but in HES for Non-Diabetic Retinopathy
- suspended from RDS for closer monitoring
- in HES for DR
- digital surveillance pathway
- slit lamp biomicroscopy pathway
- excluded (exclusions can be temporary)
- opted out
- medically unfit
- unable to have images taken
6.2 Excluded from screening
Excluded individuals are defined as eligible individuals who are not currently invited for routine digital screening and do not have their retinas checked for diabetic retinopathy in another part of the screening pathway.
This includes:
- informed opt-outs
- medically unfit/unable to have images taken
In cases where there is doubt over whether the individual should be invited or not, they should be sent an invitation. The decision to exclude a person with diabetes should only be made after careful assessment of the individual and their circumstances.
Exclusions from DES should form a very low proportion of the programme register; a national acceptable range will be determined as a baseline in the future.
Maintenance of an individual’s exclusion status should be monitored through the failsafe system via regular audits outlined in the audit schedule.
Local DES services must ensure equitable access for all eligible individuals, regardless of personal circumstances that may present barriers to attendance.
No individual should be excluded from screening due to factors that may constitute a health inequality, such as geographical distance from a screening venue or other logistical challenges.
Where such barriers are identified either directly or via the Health Equity Assessment/Audit, services must take proactive steps to offer reasonable adjustments or alternative arrangements to facilitate participation.
All decisions regarding exclusion must be based solely on clinical criteria, in line with national guidance, and must be clearly documented.
The local DES service must actively monitor exclusion patterns to ensure that no group is disproportionately affected, and that the principles of fairness, accessibility, and inclusivity are upheld throughout service delivery.
Informed opt-out
Individuals may choose to opt out of diabetic eye screening for an agreed period, up to a maximum of three years.
Local services and/or the GP (to be agreed locally) must discuss the available options with the individual, ensuring that the risks and implications of not attending screening are clearly communicated and fully understood. Individuals should be encouraged to opt-out for the shortest time appropriate.
The individual must be informed that opting out of the DES service will result in the cessation of future invitations or reminders for screening for the specified period. It must be emphasised that the individual can rejoin the DES service at any time.
Local services must ensure that all discussions and decisions are documented in the individual’s screening record.
To confirm an informed decision, the individual must submit their request to opt out either by email or in paper form, with a copy retained in their record. In exceptional cases where an individual is unable or unwilling to submit their request by email or paper form, alternative methods of confirmation may be used, provided these are documented in the individual’s record. DES services should develop a local policy which details the opt out process.
The opt-out correspondence must be retained by the local DES service in accordance with NHS records retention guidelines. A confirmation letter should be sent to both the individual and their GP, clearly stating that the individual has opted out of screening for the requested period.
After the opt-out period concludes, the DES service will automatically send a new screening invitation to the individual unless updated opt-out information is received.
Medically unfit
Medically unfit covers the following categories of people:
Terminally ill
Terminally ill individuals should still receive screening invitations, with decisions about attendance made by themselves/authorised advocate or their medical/care team.
Pre-existing conditions
Individuals who are unable to receive or benefit from treatment due to a pre-existing condition should be evaluated by their wider medical/clinical team.
The pre-existing condition determines which medical/clinical team is most appropriate to decide if the individual should be classed as medically unfit and excluded from screening. The pre-existing condition may be ocular, or non-ocular related therefore the DES clinical lead may not be best placed to exclude the individual from screening. This should be determined on an individual basis.
If the medical/clinical team for the individual confirms this status, they should be classified as ‘medically unfit’ and excluded accordingly. The individual concerned should be informed they will be excluded from screening.
An individual should have their ‘medically unfit’ status removed if the pre-existing condition changes and they are able to benefit from screening.
When images cannot be taken
Separate guidance should be utilised when determining if an individual should be excluded when images cannot be taken at the point of screening.
6.3 Suspended from RDS for closer monitoring
Suspended individuals are defined as eligible individuals who are not currently invited for routine digital screening but continue to have their retinas checked for diabetic retinopathy in another part of the screening pathway or within HES
This includes being:
- under the care of the HES for management or treatment of DR
- unable to be assessed in a screening environment but can be assessed in HES
- under surveillance in the DES Slit Lamp Biomicroscopy (SLB) pathway
- under surveillance in the DES Digital Surveillance and OCT pathway
- Under surveillance due to pregnancy
6.4 Ineligible for screening
Individuals ineligible for screening are those who are recorded in the DES software within a local DES service but should not be invited for screening as they have no perception of light in both eyes and would not benefit from DES or treatment for DES.
7. Off register
This group of people are present on the database of the screening programme, but their current status means that they should not be included as ‘on register’ and therefore cannot be sent an appointment for screening by that local DES (they may be offered screening in another DES)
This includes people who:
- are deceased
- moved out of area
- refused demographic transfer but known to DESP (see section 9)
- are screened in another DES service
- are not diabetic/diabetes resolved
- under 12
These individuals should be classed within the DES software as off register. The decision and supporting evidence for this status must be documented within the screening software to provide assurance that the individual’s status is correctly recorded if appropriate.
8. Postponement of DES appointments
If an individual is invited for screening but requests to temporarily delay their appointment, it can be postponed for a maximum period of six months at a time.
The opt-out process should not be used for this purpose.
Individuals must be informed of the risks associated with postponing their appointment and advised that they will automatically be re-invited for screening at the end of the postponement period.
Postponements may be extended for additional periods if requested, and each instance should be documented accordingly.
During the postponement period, the individual will remain classified as active within the screening service and included in the associated performance reports.
Local DES services should not be using the postponement status to manage call/recall lists and repeated DNAs.
9. Permanent opt-out by refusal for transfer of data to screening service
Consent to send an individual’s details to the DES service is not required. Individuals who wish to permanently opt out of DES may do so by withholding or withdrawing their consent for data sharing between their GP and the local DES service. This is the only mechanism by which an individual can permanently prevent invitations and any communication from the local DES service.
Individuals must submit a formal request through their general practitioner (GP) to prevent the sharing of their data with the DES service. The GP must then document this decision in the individual’s medical record using the designated SNOMED-CT code.
The SNOMED-CT code that should be added to the individuals GP record is-
Consent to share demographic info for retinal screening withheld – 305471000000107
If this decision is made at the time of the diabetes diagnosis, prior to the individuals first inclusion on GP2DRS, they will remain unknown to the DES service. If the DES service already holds a record for the individual, their status will be updated to “off register – refused demographic transfer but known to programme.”
It is the responsibility of the GP to ensure that individuals who choose to permanently opt out of the DES programme are fully informed of the potential risks to their eyesight. The GP should also inform the individual that they can opt back into the screening programme at any time.
10. Post office returns
When a post office return is received, the service-user and their GP should be contacted to verify the current address. If the information cannot be updated, the service-user is marked as ‘Not known at this address’ within the software. The service-user remains eligible for screening but will not be invited until their address details are updated. Monthly failsafe checks should be performed on these service-users.
11. Record retention for DES services
Local DES services should develop their own records retention guidance in accordance with the NHS England Records Management Code of Practice, and the data retention/information governance policy determined by their own organisation.
DES services should appraise records for deletion once they have been held for the minimum record retention period. Services may need to liaise with their software providers to permanently delete an individual’s record following this appraisal.
12. Situations that require specific consideration
12.1 People with ungradable images
Separate guidance regarding management of people with ungradable is available.
12.2 People who have a disability or require a reasonable adjustment.
Individuals with disabilities should be able to access their local DES service. Local services must have an up-to-date Health Equity Assessment to ensure that their services are fully accessible and compliant with relevant disability discrimination legislation.
In a small number of cases, an individual may have a disability/long term condition that prevents them from being screened by digital photography. In such cases, the clinical lead must engage in a discussion with the individual (and, where appropriate, their carer and/or GP) to assess their specific circumstances and explore available options on a case-by-case basis.
It is not appropriate for either the GP or local DES service staff to exclude an individual from screening due to their disability, provided the individual has the capacity to make informed decisions regarding their participation.
To ensure compliance with the Reasonable Adjustment Digital Flag requirement, all services will need to establish a clear, local policy and processes for following the Reasonable Adjustment Digital Flag Information Standard.
12.3 Best interest decisions
An individual whose mental capacity prevents consent to screening should not be excluded or removed from a local DES service unless a ‘best interest decision’ has been taken on their behalf. In most cases, the least restrictive option is for that individual to remain in an eligible status and receive screening invitations at routine intervals. The invitations can be considered and accepted or declined on each occasion as mental capacity may fluctuate.
Local DES services will need to ensure there is evidence that any best interest decision has adhered to the principles of the Mental Capacity Act, and that all relevant factors, reasonable adjustments, and alternatives have been considered/offered.
In exceptional circumstances, a care team may decide it is in the best interests of a person who lacks mental capacity to withdraw from a local DES service. Screening staff should be satisfied that the best interest decision has been reached in accordance with their local code of practice.
The person making the best interest decision to exclude a person from screening should be aware that the person can be re-invited at any time if circumstances change and screening is then considered to be in the person’s best interests.
12.4 Housebound People
DES and ophthalmic assessment/treatment require specialised, non-portable equipment that cannot be used in a residential environment.
Domiciliary assessment or home visits are not part of the diabetic eye screening programme.
Individuals in residential care or classified as housebound, but who can attend appointments with assistance, should still be invited for screening. Screening must remain accessible in compliance with disability discrimination laws.
Local DES services should work with the individual’s GP and where appropriate, residential care home staff to ensure people are encouraged and able to attend for screening and subsequent treatment if necessary.
People who are unable to travel outside their residence who have a disability that would preclude treatment should be assessed in line with the medically unfit process as outlined within this guidance.
12.5 Private patient access to DES
Individuals who attend private ophthalmologists should continue to be invited for screening unless they complete the opt out process to exclude them from screening.
Individuals who are registered with a private GP for the management of their diabetes and are not registered with an NHS GP will not usually be able to access screening as part of the NHS Diabetic Eye Screening programme.
12.6 People in secure settings
All eligible individuals in secure and detained settings, including prisons, immigration removal centres, and children and young people’s secure settings must have access to DES. Local services are required to establish a policy and process outlining how these individuals are identified and how they can access screening.
This may involve the service visiting the secure and detained settings on a regular basis. Alternatively, individuals may attend existing screening clinics, in which case local arrangements for transport, escorts, and other logistical considerations must be agreed upon with the relevant secure setting management.
As GP2DRS does not currently provide data for individuals in secure settings, local services must implement a process to identify eligible individuals within these environments.
12.7 Children and young people with diabetes (12–25-year-olds)
Uptake of screening is lower in this group of individuals and local Children and Young People (CYP) diabetes or care teams can have varied access to DES records for this group of individuals.
To support CYP teams and potentially improve uptake and understanding of screening within this age range, local DES services should have contact details for the CYP diabetes or care team within the service user’s record. All screening outcomes and results, including when they have not attended, should also be sent to this team as well as the individual’s GP.
12.8 People unaware of their diabetes diagnosis
GPs are responsible for informing individuals when they have received a definitive diagnosis of diabetes and providing appropriate information on diabetes management. They are also responsible for notifying the relevant clinical services about an individual’s diabetes status.
Because data of individuals coded as diabetic on GP practice software systems are automatically sent via GP2DRS to the local screening service, some people may be invited for eye screening before being notified of a confirmed diabetes diagnosis by their GP.
If an individual is unaware of their diabetes diagnosis, screening staff should advise the individual to consult their GP. The individual may choose to delay or reschedule their screening appointment accordingly.
DES pathway standards related to timely offer of screening for individuals who are newly diagnosed with diabetes still apply.
12.9 People not eligible for NHS treatment
Primary care services are free of charge to all migrant/overseas visitors to the UK, whether registering with a GP as an NHS patient, or accessing NHS services as a temporary patient.
A temporary patient is someone who is in the area for more than 24 hours and less than 3 months.
DES services should be aware that if an individual who is ineligible for NHS treatment (outside of primary care) is identified through screening as having referable disease, they may not be eligible for free of charge HES/secondary care. Individuals should be made aware of this prior to undertaking any screening to ensure an informed choice is made regarding whether to proceed or not.
DES is commissioned by the Public Health Section 7a Commissioning Teams for eligible individuals registered with a Primary Care GP. Any decision not to offer screening to individuals who may not be eligible for free treatment must be made in conjunction with the service commissioners to ensure equitable access to screening is being maintained.
Further guidance is available here: NHS entitlements: migrant health guide - GOV.UK and Charging overseas visitors in England: guidance for providers of NHS services - GOV.UK
12.10 Gender Reassignment
Further information regarding Gender reassignment (including individuals under 18) is available on the Primary Care Support England website.
Please note this guidance is under review and may be expanded to provide specific DES guidance at a future date.
12.11 Sensitive (S) Flag Status
Information on Sensitive flag status is available on the Primary Care Support England Website. An individual may have a sensitive (S) flag associated with their health record. This ensures people at risk for any reason cannot have their health information easily accessed by health professionals and the S-flag is usually added by the individual’s GP.
If individuals with an S-Flag status are highlighted through the GP2DRSextract and the individual is unknown to the DES service, they should contact the individual’s GP to determine what level of information is available and if there is sufficient information available to enable access to the screening programme.
If the individual is known to the screening programme and has a sensitive flag added to their record the local service should still invite them for screening.
Further clarification about an individual’s status can be obtained by contacting the National Back Office team.
12.12 Aggressive individuals
Occasionally a service user may become aggressive and intimidating to members of staff. In incidents such as this, to ensure staff wellbeing and dignity at work, a service may want to opt an individual out of screening for a specific period to be determined locally.
If a DES service chooses to opt an individual out of screening for this reason this must be agreed by the Clinical Lead and the individuals GP. It must also be done in conjunction with the organisation’s Violence and Aggression Prevention policy.
Full reasoning must be added to the individual’s notes and the individual’s GP must be informed in writing so that it can be included in the individual’s medical record.
13. Other types of diabetes
There are a number of other types of diabetes that carry differing risks of developing diabetic retinopathy. The NHS DES programme is not designed to provide highly specialised care for small, specific groups of individuals. Therefore, it is recommended that all individuals with other forms of diabetes are invited for routine digital screening, except for gestational diabetes. Some of the other forms of diabetes are listed below.
Individuals may opt-out of screening once they have made an informed decision, in accordance with the opt-out process outlined above.
13.1 Maturity Onset Diabetes of the Young (MODY)
An individual diagnosed with MODY should be referred to the DES programme and invited for routine digital screening, irrespective of the type of MODY they have.
13.2 Steroid induced diabetes
An individual diagnosed with diabetes due to steroid treatment should be appropriately coded by the GP and will be referred to the DES service for routine digital screening via GP2DRS.
DES screening should continue until the cessation of steroid treatment or referral to hospital eye services.
Following cessation of steroid treatment:
- if the individual shows continued signs or symptoms of diabetes, they should receive ongoing eye screening
- if there are no clinical signs or symptoms of diabetes they should be categorised as ’not diabetic’ as per this guidance
This decision should be made by the individual’s medical team and the appropriate coding applied to their GP record. If an individual had a screening outcome of R1 or worse, they should continue to be invited for diabetic eye screening.
Local services do not have to undertake any additional failsafe for service users with steroid induced diabetes. However, when they no longer appear on the GP2DRSextract, DES services should undertake standard validation checks.
13.3 Gestational diabetes
When an individual is diagnosed with diabetes during pregnancy, the clinicians involved with their care must decide whether they diagnose Type 2 diabetes or gestational diabetes.
If the clinicians diagnose gestational diabetes, no screening is required during pregnancy.
If the clinicians diagnose Type 2 diabetes during pregnancy, the service user should be coded as having diabetes by their GP practice and will be issued an invitation to attend DES screening as outlined in the guidance for screening during pregnancy. The service user should return to the standard screening pathway when they are no longer pregnant.
14. Early worsening phenomenon
The early worsening phenomenon can occur when a person with diabetes has a sudden improvement in their diabetes management, resulting in a rapid, substantial drop in a person’s HbA1c. This may lead to an increased risk of diabetic retinopathy development and progression. This can be for several reasons and includes, but is not limited to:
- a person with diabetes becomes pregnant following a poor history of control and their control improves dramatically
- commencement of insulin therapy following poor control with tablet therapy
- rapid improvement in control following initial diagnosis
- commencement on insulin pump/hybrid closed loop (HCL) therapy*
- bariatric surgery
- pancreatic transplant
- weight loss injections*
- commencement of GLP1/GIP receptor agonists*
*Evidence for the early worsening phenomenon in these cases is under review.
These individuals should be entered onto the appropriate screening interval for their pathway within the screening programme based on severity of disease; they do not require an increased frequency of screening if in the Routine Digital Screening or Digital Surveillance pathway, excluding the exception outlined below.
If an individual is due to be initiated on an HCL/GLP-1/GIP receptor agonist and did not attend their last screening appointment, they should be reinvited for screening at the request of the diabetes team, HES or GP to assess their current retinopathy status.
Individuals who are newly diagnosed with diabetes must have their diabetes diagnosis coded on their GP health record before they can be identified by GP2DRS and invited for their initial appointment via the local DES service.
If an individual under the care of the HES for diabetic eye disease requires additional retinal photography/imaging due to clinical reasons associated with their diabetes this must be undertaken with the oversight of their diabetes team and ophthalmologist within the HES. Local DES services should not undertake additional surveillance/screening appointments for this group of people.
The only exception to this is when a person with diabetes is on a 24-month recall and has had been initiated on HCL. Local DES services can utilise the ‘Clinical Lead 24-month override option’ available within the diabetic eye screening software to enable an additional screen following initiation of HCL system (this additional screen should take place 6-12 months following initiation of HCL). Local DES services are not required to additionally failsafe these individuals.
This process should only be used where the diabetes clinical team has notified the screening service clinical lead that an individual is at higher risk. If the screening result is R0M0 following this additional screening appointment the individual will automatically return to a 24-month screening interval.
Additional screening or surveillance should not be offered by DES programmes for people with diabetes being initiated on or monitored whilst on a GLP-1/GIP RA treatment. Diabetic eye screening is a population level based public health system and not designed for individualised care. Any specific individualised imaging or assessment requested by their diabetes care team should be undertaken under the care of ophthalmology within HES.
Local DES services should ensure that diabetes care teams have appropriate and timely access to screening results; this should be determined locally.
NB, all pregnant women with diabetes will be offered appropriate surveillance as part of the pregnancy pathway for DES.
15. Diabetes in remission and diabetes resolved
All eligible individuals who have previously had a definitive diagnosis of diabetes should be invited for screening for life. This is because there is still an increased risk of sight loss even if diabetes is deemed in remission (with the exceptions outlined in this guidance).
It is essential that the correct coding is applied to the GP records of these individuals. An incorrect code could lead to a person with a previous definitive diagnosis not being identified for screening.
Local DES services must verify the accuracy of the absence of individuals from the GP2DRS extract due to changes in diabetes status as part of the missing people guidance in section 3.1.
15.1 Diabetes in remission
The GP code for ‘Diabetes in Remission’ should be applied to individuals who were previously diagnosed with diabetes but no longer meet the diagnostic criteria due to a reduction in blood glucose levels (HbA1c). This remission may result from interventions such as bariatric surgery, pancreatic transplant, or significant weight loss. These individuals are included in the cohort provided by GP2DRS and should still be invited for screening for life.
15.2 Diabetes resolved
The use of “Diabetes Resolved” codes is not appropriate for individuals whose diabetes is in remission or whose blood glucose levels are within normal limits due to an intervention. It has historically been used when an individual has been incorrectly diagnosed as having diabetes and requires this to be removed from their record. Practices may still use it for this purpose; however, the correction can also be made by marking the incorrect code as ‘in error’ instead.
When an individual’s latest dated SNOMED-CT code is “Diabetes Resolved” or if all incorrect diabetes code are marked in error and removed, they will no longer be eligible for screening, and they will be excluded from the GP2DRS extract. In such cases, local DES services must verify with the GP that there was an intention to remove the patient from cohort and why (keeping notes), to ensure the coding changes have not been mistakenly applied as part of ongoing validation.